Diagnosing Lyme Disease & Tickborne Diseases in Vermont
Below is the content from a printable guide to support Vermont healthcare providers in diagnosing Lyme Disease. This online version links directly to references. Download and print a pdf, or contact VTLyme to have a printed copy sent to you.
Disclaimer: This guide is not meant to be definitive. It covers basic information about tickborne diseases in Vermont, with a focus on symptom recognition and the diagnosis of tickborne illnesses by licensed healthcare providers. Additional, comprehensive resources including those developed by the Centers for Disease Control and Prevention should be utilized along with this guide.
Dedication
To Julie Gagnon Prior, who’s singular efforts made the creation and free distribution of this guide and flowchart possible. Her courage and strength are inspirational to many Vermonters affected by tickborne illnesses.
 The long term impact of tickborne diseases on Julie’s health was preventable. It is her hope that no more Vermonters will experience health problems as a result of delayed diagnosis, misdiagnosis, or inadequate treatment of a tickborne illness.
The long term impact of tickborne diseases on Julie’s health was preventable. It is her hope that no more Vermonters will experience health problems as a result of delayed diagnosis, misdiagnosis, or inadequate treatment of a tickborne illness.
In 2020, Julie created the VT Pin Up Girl Calendar donating 100% of funds raised to help Vermont’s health care providers better recognize, diagnose and treat tickborne illnesses.
Introduction
Tickborne diseases are a rising national epidemic. Vermont often has the highest rate of Lyme disease in the USA, and ticks in Vermont can transmit other diseases too. Lyme disease is most prevalent, though patients can be infected with multiple tickborne pathogens at the same time with or without Lyme disease, including Anaplasmosis, Babesiosis, Ehrlichiosis, and Borrelia miyamotoi.
Diagnosing a tickborne illness is challenging; symptoms can be variable, disease timing and progression may differ in each patient, testing can be inaccurate, and a history of controversies about diagnosis and treatment confuses both providers and patients.
One thing universally agreed upon is that early and accurate diagnosis, and effective treatment, can help prevent a tickborne infection from becoming complex and causing ongoing health problems.
This manual was created to help Vermont’s healthcare providers accurately diagnose Lyme and tickborne diseases. This is a very basic guide to diagnosis, therefore use of additional, comprehensive resources is recommended and encouraged.
Until laboratory detection of tickborne diseases improves, clinical settings remain the most important place for Vermonters to access correct diagnosis and effective treatment. A practitioner’s ability to accurately and promptly diagnose a tickborne infection is the first step to preventing adverse clinical outcomes and ongoing health complications resulting from delayed diagnosis of a tickborne illness.
With Vermont’s children being at highest risk for Lyme disease it is also critical to understand how pediatric tickborne illnesses can present as cognitive, behavioral, or learning problems. In both children and adults, mood lability, memory problems, or a change in behavior may be the only symptom of a tickborne disease.
Vermonters need health care providers educated about the diagnosis of tickborne diseases. Thank you for taking the time to consult this guide and educate yourself about the diagnosis of Lyme and tickborne diseases.
10 Important Points about Lyme and Tickborne Diseases (TBD) in Vermont
- People can be infected with more than one tickborne pathogen at the same time. Some require different treatments.
- According to Vermont Department of Health data almost 40%, of Vermonters with confirmed Lyme disease did not have a “bulls-eye” rash. Other TBDs do not present with a rash.
- Serology will not detect all cases of tickborne disease. A negative blood test does not necessarily confirm a patient does not have a tickborne disease.
- There are three stages of Lyme disease; almost all peer reviewed research on testing and treatment outcomes was done on subjects in the early, first stage of disease.
- Lyme disease is diagnosed all 12 months of the year in Vermont.
- According to the CDC, many patients with a tickborne disease do not remember being bitten by a tick. Remembering a tick bite is not a requirement for a TBD diagnosis.
- 10-20% of patients treated for Lyme disease can have ongoing symptoms for months after treatment.
- In some patients, tickborne illnesses have presented as mental health disorders, cognitive difficulties, or behavioral changes. Research has shown a link between suicidality and neurological Lyme disease.
- While some tickborne diseases are not established in Vermont, frequency of travel means it is important for a clinician to be familiar with the signs and symptoms of a variety of TBDs.
- The psychosocial impacts of a complex tickborne illness can be driven by neurological symptoms, mood disorders, relationship problems, insomnia, cognitive difficulties, change in work/school performance, loss of employment, memory loss, financial difficulties and more. A comprehensive view of a patient’s health should be considered when treating complex tickborne illnesses.
Treatment
There are different approaches to the treatment of Lyme disease. Peer reviewed guidelines published by the Infectious Diseases Society of America (IDSA) and the International Lyme and Associated Diseases Society (ILADS) can be consulted to decide the best treatment for your patient.
A note about the importance of early diagnosis in Lyme disease: Almost all published studies on treatment outcomes have been done on subjects in Stage 1 of Lyme disease who received early diagnosis and treatment. It is unlikely this research accurately reflects disease progression or outcomes in patients diagnosed in the second or third stages of Lyme disease, or who have Lyme comorbid with other tickborne pathogens, bartonella, mold/mycoplasma, or viruses.
Amidst ongoing controversy about the etiology and treatment of Post Treatment Lyme Disease, there is agreement that early diagnosis and effective treatment likely prevent complex health problems related to a tickborne illness and improve patient outcomes.
TBD Diagnosis Overview
- Clinically diagnosing a tickborne disease can be challenging.
- Symptoms of one TBD can be similar to those of other illnesses.
- Patients may not remember having a tick bite.
- Symptom onset can happen days, weeks, months or years after initial infection, so even patients who remember a tick bite may not connect the incident with their symptoms or illness.
- Patients may have more than one TBD.
- Sometimes a patient will present with a fever and clear erythema migrans, making a clinical diagnosis of Lyme disease straightforward. Yet, a provider must consider that any patient exposed to an infected tick may have also contracted another TBD such as Babesia, requiring different treatment.
- Tickborne diseases are diagnosed all 12 months of the year in Vermont
- Mostly in the spring and summer months.
- Many Vermonters don’t realize that risk of infection (especially anaplasmosis) increases again in October and November as ticks look for one more blood meal before winter.
- This activity unfortunately coincides with hunting season in Vermont, so it is important patients are aware of the continued need for tick bite prevention even after summer ends.
- Blood tests for some tickborne diseases are not conclusive.
- According to the CDC, tests for Lyme disease can be negative in the first 4-6 weeks of infection as the body develops antibodies.
- This can be a critical time for a patient to receive treatment in the early stage of disease.
- Testing in later stages may not be accurate, and tests are not available for some TBDs. The Vermont Department of Health notes, “Even the best available Lyme testing is imperfect.”
- Clinical judgment is paramount for effective treatment.
- Because Vermont has among the highest rates of Lyme disease in the USA, along with rising rates of other tickborne diseases, health care providers should be familiar with the nuances of diagnostic testing and disease symptoms.
- Because the diagnosis and treatment of tickborne diseases is an emerging science, not one that has been settled by comprehensive and cohesive research, clinical judgment is paramount. Educating yourself with equitable information about tickborne diseases is a vital part of effectively caring for patients who trust and rely on your expertise and insight.
Diagnosing Lyme Disease
Of multiple tickborne pathogens are present in Vermont Borrelia burgdorferi is the most prevalent found in about 60% of blacklegged ticks in Vermont. While this section of the manual focuses on Lyme disease because it is the most prominent TBD in Vermont, Vermonters can be infected with other tickborne pathogens with or without the presence of Lyme disease. See the following sections and the CDC’s Tickborne Diseases of the United States, A Reference Manual for Healthcare Providers as a resource for information about TBDs in Vermont and in neighboring states.
Understanding the Stages of Lyme Disease
Lyme disease has 3 Stages: 1.Early Localized, 2.Early Disseminated, 3.Late Disseminated
- Early Localized
Signs and symptoms of Early Localized (acute) Lyme disease usually begins days or weeks after a tick bite. The infection has not spread throughout the body yet, and symptoms may include rash, fever, fatigue, headache, stiff neck, sore muscles, joint pain, sore throat, or swollen lymph nodes.
- Early Disseminated
Early Disseminated Lyme disease mostly occurs weeks or months after a tick bite. Bacteria begin to spread throughout the body. Additional symptoms may include chills, pain in the arms or legs, weakness, vision changes, heart palpitations, chest pain, rash, depression or mood disorders, memory problems, Bell’s palsy, nausea or vomiting.
- Late Disseminated
Late Disseminated Lyme disease can occur weeks, months or years after a tick bite. Patients may develop chronic arthritis, cognitive and neurological problems, and cardiac symptoms. Other symptoms may include: insomnia, vertigo, severe headaches/migraines, numbness in legs and arms, severe fatigue, processing speed difficulties, stiff neck, vision or auditory problems, myalgias, mood lability, “brain fog,” mental health disorders, Bannwarth’s syndrome, and gastrointestinal disorders. In children, some of these symptoms may mimic learning disabilities.
Clinical Diagnosis of Lyme Disease
Symptoms of Lyme disease can be similar to other diseases, making diagnosis challenging. Diagnosis should be based on a patient’s symptoms, medical and behavioral history, and tick exposure. (Since Vermont is an endemic state, most Vermonters could be considered to have a “history of tick exposure.”)
Blood tests can provide evidence supporting a clinical diagnosis, but should not be considered definitive. The CDC directs health care providers to consider patient history, symptoms, and timing to accurately order a test and interpret test results. The General Symptom Questionnaire (GSQ-30) has been shown to be a reliable instrument to assess symptom burden among patients with acute and post-treatment Lyme disease syndrome and is sensitive in the detection of change after treatment among patients with erythema migrans.
“Symptoms of disseminated Lyme disease can occur days to months after the initial infection” – VDH
Symptoms may include one or more of the following
- Fatigue
- Chills and fever
- Muscle and joint pain (often migrating – appearing in different places in the body)
- Headache
- Swollen lymph nodes
- Tiredness
- EM rash or Atypical EM rash
According to the Vermont Department of Health, Lyme disease may spread to various parts of the body. This is called “disseminated Lyme disease.”
Symptoms associated with disseminated Lyme disease:
- Numbness and pain in the arms or legs
- Paralysis of facial muscles (usually on one side of the face, also known as “Bell’s palsy”
- Fever
- Stiff neck
- Severe headaches
- Abnormal heart beat
- Joint pain and swelling
- Meningitis
- Chronic nervous system problems
- Shooting pains
- Numbness or tingling in the hands and feet
- Problems with concentration and short-term memory
Blood Tests Explained
Facts about Blood Tests for Tickborne Diseases
- According to the CDC, tests for tickborne diseases can be negative for 4-6 weeks after infection.
- Test results can vary among different laboratories or different test kits.
- Serology will not detect all cases of tickborne disease.
- Prophylactic and other antibiotic treatment can cause an infected patient to test negative.
- Most Lyme disease testing research has been on subjects with erythema migrans (EM), and may not reflect the situation of patients without EM (>30% of Vermonters), or patients with later stage illness.
- Each different tickborne disease requires its own test. For example, if a patient tests negative for Borrelia burgdorferi they could be positive for Borrelia myamotoi, but this requires a different test.
- According to the CDC providers who diagnose a tickborne disease based on their clinical judgment should begin treatment, not wait for a patient’s test results.
- It is important Vermont healthcare providers understand the limitations of laboratory testing to ensure patients infected with one or more tickborne pathogens are accurately diagnosed and receive proper treatment, as some of these diseases have the potential to cause disabling illness or death.
Lyme Disease Testing Research
The majority of research that shows effectiveness of laboratory testing and treatment for Lyme disease was done on subjects who presented with erythema migrans, and who were tested and treated in the early stage of disease. Studies on patients in later stages of Lyme disease, and research on other tickborne diseases, is extremely limited. It is important for practitioners to understand that published research may not reflect the circumstances of many Vermonters.
Health care providers cannot always rely on a blood test to determine whether or not their patient has Lyme disease. Peer-reviewed studies show that serological tests have, “limitations related to how the human immune system reacts to infection with B. burgdorferi.” UVM infectious disease specialist Dr. Dean Dejace notes, “even the best Lyme testing is imperfect and should be interpreted in the context of the patient’s clinical presentation.” There are also concerns about test accuracy for other tickborne diseases, making clinical judgment paramount.
Note: according to the CDC, blood tests for Lyme disease are likely to be negative in an infected patient in the early weeks of infection. “If a patient has a rash that is not typical of EM, a positive serologic test result will support the diagnosis of Lyme disease because of the high specificity of the test. Nevertheless, a negative test result for such a patient, even with an improved test sensitivity of 63%, may not reduce the probability of Lyme disease sufficiently to rule out the diagnosis.”
For Lyme disease, the CDC’s current recommendation is a 2-tiered testing procedure. The first ELISA test looks for antibodies that respond to Lyme-causing bacteria. If a patient is positive they are given an immunoblot to validate the ELISA and reduce the chances of false-positive results.
One difficulty with this process is that a negative test could mean a patient does not have Lyme disease, but it could also mean they had an atypical immune response or that the test was done too early. Because there are multiple strains of Borrelia worldwide, and each test looks for a specific strain, it can be possible to miss a tickborne infection by not ordering the correct test. According to Stanford University researchers, Lyme disease testing guidelines “predated a full understanding of key B. burgdorferi antigens and have a number of shortcomings.”
Tick Testing
There are different opinions about whether to have a tick tested for pathogens. The VDH and CDC discourage using results from these tests to guide decisions about diagnosis or treatment because even if a tick contains a germ, it does not mean that a patient has been infected. Also, a negative results can be misleading because your patient might have been bitten unknowingly by a different, infected tick.
Some patients may choose to have the tick tested immediately. Others may decide to save the tick in a plastic bag in a freezer (labeled with the date and location the tick was found and removed). Then, if symptoms of a tickborne disease arise, testing the tick is possible when more information is needed.
PTLD/PTLDS
According to the CDC, “Although most cases of Lyme disease can be cured with a 2- to 4-week course of oral antibiotics, patients can sometimes have symptoms of pain, fatigue, or difficulty thinking that lasts for more than 6 months after they finish treatment.” The CDC calls this “Post Treatment Lyme Disease Syndrome” or PTLDS. Because symptoms are ongoing, this condition is also called “Post Treatment Lyme Disease” (PTLD), Lyme+ or Complex Lyme. Some patients may refer to this as “Chronic Lyme.”
PTLD symptoms may include “incapacitating fatigue, chronic pain and neuro-cognitive impairment. Symptoms are often so severe that normal schedules for work, school, and personal lives are derailed.” Studies show treatment failure rates for Lyme disease may range from 10% to 20%. Because most of these studies were done on patients diagnosed and treated early in the first stage of Lyme disease, the rate for patients diagnosed in second or the stages of Lyme disease may be higher. Incidence of PTLD has increased in the US from 2016 to 2020.
The CDC notes three possible causes of PTLD:
- An ongoing auto-immune response triggered by Borreliaburgdorferi
- A persistent but difficult to detect infection
- Other causes unrelated to the patient’s Borrelia burgdorferiinfection
With no definite cause or treatment for PTLD, patients rely on the expertise of their medical providers.
Because 10-20% of patients treated for Lyme disease may experience PTLD, it is important that providers schedule follow-up visits and monitor their patients for symptoms such as increased fatigue, neurocognitive impairment paresthesia, or dysesthesia, depression, or joint or muscle pain.
Mental Health and TBD
Anxiety, depression, OCD, outbursts of rage, mood swings, memory loss, personality changes and cognitive difficulties can be related to Lyme and other tickborne diseases. While a mood disorder may be unrelated to an illness, or a reaction to being ill, it is also possible that infection may be the biological cause.
Dr. Brian Fallon, director of the Lyme Disease Research Program at Columbia University, suggests these warning signs of Lyme encephalopathy:
- Are there markers of non-psychiatric disease such as erythema migrans rash, arthralgias or arthritis, myalgias, headaches, sound or light sensitivity, paresthesias, tremors or twitching, cardiac palpitations, word-finding problems, short-term memory loss, cranial neuropathies, radicular or shooting pains?
- Is the psychiatric disorder atypical or unusual? For example, does a panic attack last longer than the expected 1/2 hour? Or is it a first ever panic attack at age 50?
- Is there poor or paradoxical response to psychotropic medications, or excessive side effects/sensitivity to these medications?
- Is this new-onset disease without psychological precipitants such as new stressors or secondary gain?
- Is there an absence of a personal history or family history of major psychiatric disturbances?
“Negative answers to these questions do not rule out the presence of Lyme disease and co-infections. But a “yes” to most of these questions, especially in a patient with an out-of-doors lifestyle or a pet, demands further clinical assessment.”
Pediatric TBD
Tickborne diseases can manifest differently in children. Young children may not be able to recognize or describe their symptoms, and behavioral or cognitive changes may be the only signs of a tickborne illness. In adolescents, symptoms such as mood swings, depression, insomnia, anxiety, or poor executive function may be attributed to developmental changes. It can be challenging for clinicians, educators, and parents/caregivers to look past acute behavioral manifestations to an underlying cause.
The onset of a child’s tickborne illness may be gradual, with subtle cognitive or neurological changes, increasing fatigue, changes in peer relationships, and deteriorating academic performance. Uncharacteristic behaviors can be misinterpreted as oppositional or manipulative, making it difficult for a sick child to get accurate diagnosis and effective treatment.
Psychosocial Impact
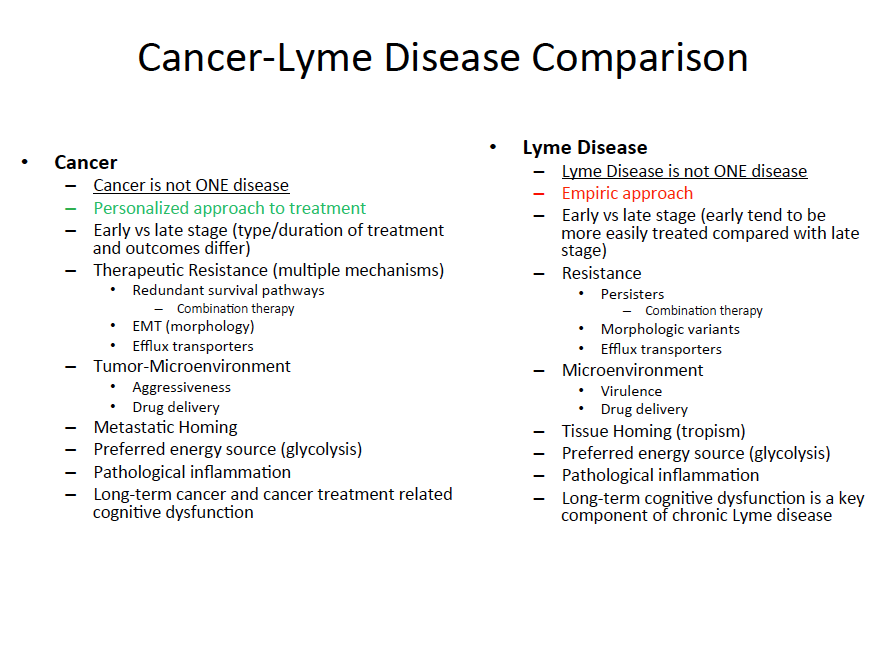
Dr. Neil Spector has described Lyme disease as “the infectious disease equivalent of cancer” due to its potential complexity and the need for an individualized treatment approach. Vermonters with a complex tickborne disease need understanding, support, and access to care. In addition, early diagnosis and effective treatment may prevent ongoing health and related psychosocial complications.
{kind=link}
People with complex, ongoing health problems related to Lyme or tickborne diseases may not appear ill even when their physical pain is extreme or personal experiences extremely difficult. may experience job loss, relationship difficulties, loss of social support, changes in work/school performance, disability, divorce, and financial problems.
Studies have shown “There is considerable impairment of health-related quality of life among patients with persistent symptoms despite previous antibiotic treatment for acute Lyme disease”. A study by Klempner, et al., and patients can experience symptoms “Months to years after the initial infection with B. burgdorferi.” A study by Steere, et al.,
A recent study showed the quality of life for post-treatment Lyme patients was lower than patients with other chronic diseases, “including congestive heart failure, diabetes, multiple sclerosis and arthritis”. In addition, these patients had, “significantly lower health quality status, more bad mental and physical health days, a significant symptom disease burden, and greater activity limitations” when compared to the general population. They also reported “impairment in their ability to work, increased utilization of healthcare services, and greater out of pocket medical costs”. The National Institute of Allergies and Infectious Diseases noted these studies “reinforced the evidence that patients reporting PTLDS symptoms have a severe impairment in overall physical health and quality of life”.
When a Patient Has Multiple Tickborne Infections
A patient may have more than one tickborne illness at the same time. Other bacteria, protozoa, and viruses carried by ticks are present in Vermont along with the bacteria causing Lyme disease and comorbidity may increase the complexity of a patient’s illness. Tests for a specific TBD, like Lyme disease, will be negative if the patient is infected with a different tickborne disease(s). Signs and symptoms of these illnesses may overlap, confusing the diagnostic picture. For additional information refer to the CDC’s Tickborne Disease Reference Manual for Healthcare Providers.
Tickborne Disease Diagnosis BASICS
Below is a basic overview of tickborne diseases in Vermont with information from the CDC and the Vermont Department of Health. Additional, comprehensive information can be found at these and other sources.
Some tickborne diseases can be severe and even fatal if left untreated so it is important for health care providers to be aware of the wide range of symptoms, and atypical presentations, of tickborne illnesses.
Remember, it is possible for a patient to contract a single disease, or multiple infections simultaneously. All of these pathogens are present in Vermont.
Anaplasmosis
The bacterium Anaplasma phagocytophilum causes anaplasmosis. In Vermont the most common symptoms reported include fever, malaise, muscle aches, chills and headaches.
Symptoms of anaplasmosis usually begin five to 21 days after a tick bite. Other symptoms include cough, confusion, and nausea/vomiting. People with anaplasmosis can develop anemia, low white blood cell counts, low platelet counts, and elevated liver enzymes.
Anaplasmosis does not usually cause a rash.
Like Lyme disease, the risk for contracting anaplasmosis is highest during summer months. However, unlike Lyme disease, the risk for anaplasmosis significantly increases again in autumn.
According to the CDC, the standard serologic test for diagnosis of anaplasmosis is the indirect immunofluorescence antibody (IFA) assay for immunoglobulin G (IgG) using A. phagocytophilum antigen. Antibody titers are frequently negative in the first week of illness. Anaplasmosis cannot be confirmed using single acute antibody results. Although a positive PCR result is helpful, a negative result does not rule out the diagnosis, and treatment should not be withheld due to a negative result.
Babesiosis
Babesiosis is caused by a microscopic blood parasite called Babesia microti.
Symptoms of babesiosis usually begin one to four weeks after a tick bite. These can include fatigue, fever, chills, night sweats, head and body aches, decreased appetite, and nausea. Babesiosis can also cause hemolytic anemia. Some people who have been infected with Babesia experience no symptoms.
Babesiosis can be diagnosed by blood smear or antibody testing. It is important to note that antibody testing for B. microti will not show evidence for other Babesia species. I babesia is suspected, patients who are negative for B. microti can be given a separate test for Babesia duncani or other antibodies.
With Babesia, a CBC may show decreased red blood cells, thrombocytopenia, and a normal (or slightly decreased) white blood cell count. CMP results may include Increased creatinine level, increased BUN level, increased liver enzymes, ALT and AST, and lactate dehydrogenase (LD) levels consistent with an infection and parasites in the blood.
Vermonters’ risk for Babesia is highest June through August, but exists anytime blacklegged ticks are active.
Borrelia miyamotoi
Borrelia miyamotoi is related to a bacteria that causes tickborne relapsing fever (TBRF). Symptoms of a Borrelia miyamotoi infection include fever, chills, muscle aches, fatigue, joint pain and headaches. The fever may come and go (“a relapsing fever”). Borrelia miyamotoi infection does not usually cause a rash.
Borrelia miyamotoi sounds similar to the bacteria that causes Lyme disease (Borrelia burgdorferi) but tests used to diagnose an infection with Borrelia burgdorferi will not work for a Borrelia miyamotoi infection.
According to the CDC, “serologic testing for tickborne relapsing fevers is not standardized and results may vary by laboratory.” Like Lyme disease, serum taken early in infection may be negative. If patients have traveled out of state a different Borrelia species may be involved.
Other laboratory findings may include normal to increased white blood cell count with a left shift towards immature cells, a mildly increased serum bilirubin level, mild to moderate thrombocytopenia, elevated erythrocyte sedimentation rate (ESR), and slightly prolonged prothrombin time (PT) and partial thromboplastin time (PTT).
Ehrlichiosis
Ehrlichiosis is caused by an infection with one of several species of Ehrlichia bacteria. These bacteria are ususally transmitted by the lone star tick (Amblyomma americanum) and the blacklegged tick (Ixodes Scapularis).
Symptoms of ehrlichiosis include fever, headache, chills, malaise, muscle pain, confusion, red eyes, nausea, vomiting and diarrhea. These usually begin one to two weeks after being bitten by an infected tick. A rash is not a common symptom, but can happen with Ehrlichiosis and is more common in children with the disease than in adults.
Ehrlichiosis can be fatal if not treated appropriately. Symptoms of ehrlichiosis can be non-specific and vary from person to person, making diagnosis difficult. Because treatment with antibiotics is more effective when started earlier in the illness, a prompt diagnosis based upon clinical signs and symptoms can be important. (Blood collected at the time of diagnosis can then be used to confirm the diagnosis.)
Ehrlichiosis is rare in VT but patients can be infected when traveling to other states. According to the CDC, advanced ehrlichiosis may be confused clinically with non-tickborne illnesses such as meningoencephalitis, sepsis, toxic shock syndrome, gastroenteritis, hepatitis, and blood malignancies.
Similar to anaplasmosis, the CDC recommends clinical diagnosis of ehrlichiosis and states that treatment should not be delayed pending the receipt of tests results, or withheld on the basis of an initial negative result.
The serologic test for diagnosis of ehrlichiosis is the indirect immunofluorescence antibody (IFA) assay for immunoglobulin G (IgG). Antibody titers are frequently negative in the first week of illness. Culture isolation and immunohistochemical (IHC) assays of Ehrlichia species are only available at specialized laboratories; most routine hospital blood cultures cannot detect the organism.
Lyme Disease
Lyme disease is the most common tickborne disease in Vermont. It is caused by an infection with the bacterium Borrelia burgdorferi. Early symptoms of Lyme disease often (but not always) begin three to 30 days after a tick bite and may include: Erythema migrans (EM) or other rash, fever, headache, muscle pain joint pain and fatigue.
While the EM rash is a well-known symptom of Lyme disease many Vermonters with Lyme disease do not get a rash. 2016 Vermont Department of Health data showed in almost 40% of confirmed cases of Lyme disease reported to the Vermont Department of Health, the patient did not have an EM rash at the time of their diagnosis.
Lyme disease that is not diagnosed and treated early may progress into later stages of disease with additional symptoms including: rashes, painful joints, joint swelling, Bell’s palsy, radiculoneuropathy, problems with short-term memory, carditis, meningitis/encephalitis, mental health disorders, and pain that comes and goes in muscles, joints, bones and tendons. These symptoms of second or third stage Lyme disease can appear days to years after the initial infection.
The CDC currently recommends a two-step testing process for Lyme disease. According to the CDC, patients with Lyme disease will likely test negative in the initial weeks of infection and recommends providers “initiate treatment as soon as possible, rather than waiting for laboratory results, which may be insensitive in early illness.”
It is important to note that tests for Lyme disease will not assess whether a patient has a different tickborne disease in addition to of Lyme disease. Also, Vermonters may contract another tickborne disease without contracting Lyme disease.
Rocky Mountain Spotted Fever (RMSF)
Early signs and symptoms (including fever and headache) may not be specific to RMSF. This disease can rapidly progress to a serious and life-threatening illness. Signs and symptoms may also include: nausea, vomiting, stomach pain, muscle pain, lack of appetite and skin rash.
According to the CDC, patients with RMSF usually develop a rash 2-4 days after fever begins. Rashes vary; some can look like red splotches and some look like pinpoint dots. While almost all patients with RMSF will develop a rash, it often does not appear early in illness, which can make RMSF difficult to diagnose. Providers should consider RMSF in cases of non-specific febrile illness and sepsis of unknown origin, particularly during spring and summer months when ticks are most active.
The standard serologic test for diagnosis of RMSF is the indirect immunofluorescence antibody (IFA) assay for immunoglobulin G (IgG) using R. rickettsii antigen. Antibody titers are frequently negative in the first week of illness. For more in-depth information about diagnostic testing, see the CDCs publication: Diagnosis and Management of Tickborne Rickettsial Diseases: Rocky Mountain Spotted Fever and Other Spotted Fever Group Rickettsioses, Ehrlichioses, and Anaplasmosis — United States: A Practical Guide for Health Care and Public Health Professionals
From the CDC: “The decision to initiate antibiotic therapy for RMSF should be made based on clinical signs and symptoms and a careful patient history, including a recent tick bite or exposure to areas with ticks. A confirmatory diagnosis can be established later using specialized laboratory tests. Never delay or withhold treatment pending the receipt of laboratory test results, or on the basis of an initially negative result.”
Southern Tick-Associated Rash Illness (STARI)
It can be easy to confuse STARI with Lyme disease as many of the symptoms can be similar, including an expanding “bull’s-eye” rash that develops around the site of a lone star tick bite. Other symptoms of STARI include fatigue, fever, headache, joint or muscle pains.
Because the cause of STARI is unknown, no diagnostic blood tests have been developed.
Since STARI is not caused by the same bacterium that causes Lyme disease (Borrelia burgdorferi) tests for Lyme disease will be negative, despite clinical observations that seem to indicate Lyme disease.
One study showed some clinical differences between Lyme disease and STARI. The time for a rash to develop was shorter (averaging 6 days) in STARI than Lyme disease, patients with an EM from STARI were less likely to have additional symptoms than patients with an EM from Lyme disease, and STARI patients recovered more rapidly after antibiotic treatment than patients with Lyme disease.
While STARI is called “Southern” the habitat of the Lone star tick has expanded north, and now includes certain regions of Vermont and bordering states.
Alpha Gal Allergy
Alpha-gal allergy is believed to be related to a Lone star tick bite. Alpha-gal allergy is a reaction to a sugar molecule found in mammals that are not humans or primates. Alpha-gal is found in meat and sometimes in products made from mammals such as cheese. Symptoms of an alpha-gal allergy commonly appear 3-6 hours after eating meat (e.g., beef, lamb, pork, venison, and rabbit) or exposure to products containing alpha-gal.
Symptoms include: hives, rash, difficulty breathing, drop in blood pressure, dizziness or faintness, nausea or vomiting, and severe stomach pain.
According to the CDC Alpha-gal allergies can be severe, and even life-threatening. Healthcare providers should be aware of the possibility of a severe allergic reaction. Blood tests for IgE antibodies to alpha-gal can confirm alpha-gal allergy, along with a detailed patient history and physical examination.
Other Considerations
Other factors can impact symptoms and treatment of tickborne diseases.
Bartonella
Bartonellosis, also known a ‘Cat Scratch Disease,’ is a bacterial infection. (While not known as a tickborne disease, according to Columbia University Irving Medical Center, “The evidence for ticks as vectors of Bartonella organisms is circumstantial but fairly strong.)”
Some people with a Bartonella infection are asymptomatic, while others can exhibit symptoms such as low-grade fever, tender or enlarged lymph nodes, headache, or a pustule at the site of the scratch. Less common symptoms include eye infections, severe muscle pain, encephalitis, skin lesions, and infections in the heart, liver, spleen or bones.
Immunocompromised people are more vulnerable to Bartonella infections, and comorbidity with a tickborne illness can complicate presentation and treatment. One important consideration is studies showing psychiatric symptoms of Bartonella (links below). Sudden agitation, panic attacks, treatment-resistant depression, violent outbursts, school avoidance, and sudden-onset schizophrenia.
Chronic Virus
Mold/Mycotoxin Illness
Metal Toxicity